

BCPS 2013: Vaccines
/
 Vaccines: the memorization of when and what and when not to if the patient has certain conditions. Imagine questions that are simple but complicated. For example, perhaps an age is given and you need to know what vaccinations were due by that age or if the child had never had vaccines what could be given as catch-up? It is really not complicated and again if you are a parent this may be an easier topic if you are of the pro-vax crowd (as I am).
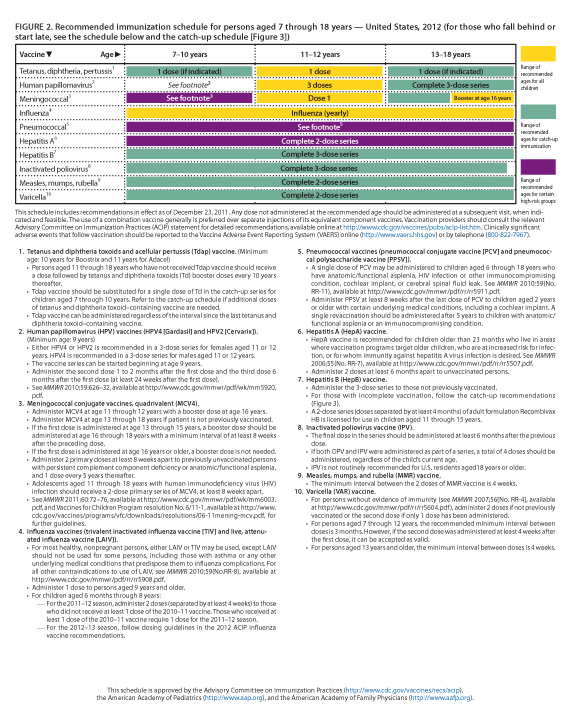
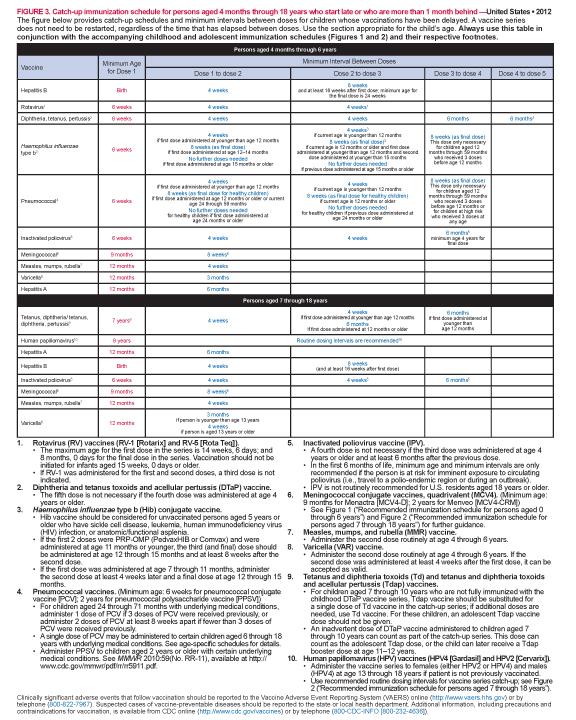
Below see the schedule from the CDC that is also approved by the American Pediatric Association along with the recommended schedule for catching up on vaccines if missed.
Vaccines: the memorization of when and what and when not to if the patient has certain conditions. Imagine questions that are simple but complicated. For example, perhaps an age is given and you need to know what vaccinations were due by that age or if the child had never had vaccines what could be given as catch-up? It is really not complicated and again if you are a parent this may be an easier topic if you are of the pro-vax crowd (as I am).
Below see the schedule from the CDC that is also approved by the American Pediatric Association along with the recommended schedule for catching up on vaccines if missed.

Special Population Considerations
1. Preterm infants
- Immunize on the basis of chronologic age.
- Do not reduce vaccine doses.
- If birth weight is less than 2 kg, delay HepB vaccine because of reduced immune response until the patient is 30 days old or at hospital discharge if it occurs before 30 days of age (unless the mother is positive for HepB surface antigen).
2. Children who are immunocompromised
- No live vaccines
- Inactivated vaccines and immune globulins are appropriate
- Household contacts should not receive oral polio vaccine
- MMR, influenza, varicella, and rotavirus vaccines are recommended
3. Patients receiving corticosteroids
a. Live vaccines may be administered to patients receiving the following:
- Topical corticosteroids
- Physiologic maintenance doses
- Low or moderate doses (less than 2 mg/kg/day of prednisone equivalent)
b. Live vaccines may be given immediately after discontinuation of high doses (2 mg/kg/day or more of prednisone equivalent) of systemic steroids given for less than 14 days.
c. Live vaccines should be delayed at least 1 month after discontinuing high doses (2 mg/kg/day or more of prednisone equivalent) of systemic steroids given for more than 14 days.
4. HIV Positive Patients
a. MMR should be administered unless patient is severely immunocompromised. b. Varicella should be considered for asymptomatic or mildly symptomatic patients. c. Inactivated vaccines should be administered routinely.

