I feel I have a bit of insight into the test and can attest to what is needed to know in each section. Keep in mind the guidelines could change between 2012 and 2013 along with the test questions, but for the most part I found the test to be incredibly fair though stressing areas more than others that I would have not expected.
I want you to pass! First attempt!
So what do you need to do to pass? Start now. I especially am talking to those with families and/or children and very little time to spare for sitting down and studying the traditional way. Again, I did fail this past year, so I will disclose that immediately, but I do believe I have insight into the test and very much plan to pass it this fall. It's a goal at this point for my own personal development.
So, ahead I will have some material presented that does come from the ACCP study material though reworded and simplified in more study form and perhaps some hints as to what was important on the test in each particular section. I am hoping to not get in any sort of trouble by doing this as far as with the BPS, so if this is not appropriate, would someone from there contact me? I do not plan on giving test questions per se' and I couldn't if I tried as there were far too many to memorize.
After two children I am convinced parts of my brain were delivered with the children as it is.
First up! PEDIATRICS!
This was always the topic that would terrify me prior to having children, but at this point besides missing one of the most common concepts of children and the very small amount of data on the test regarding pediatrics (at least in my opinion), pediatrics just doesn't seem so daunting.
Know the common pathogens of children in sepsis and meningitis.
0–1 month
- Group B streptococcus
- Escherichia coli
- Listeria monocytogenes
- Viral (e.g., herpes simplex virus)
- Coagulase-negative staphylococcus—nosocomial
- Gram (−) bacteria (e.g., Pseudomonas spp., Enterobacter spp.)
- nosocomial
1–3 months
- Neonatal pathogens (see above)
- Haemophilus influenzae type B
- Neisseria meningitidis
- Streptococcus pneumoniae
3 months–12 years
- H. influenzae type Ba
- N. meningitidis
- S. pneumoniae
> 12 years
- N. meningitidis
- S. pneumonia
Not to hard to figure out correct? Keep in mind that H. flu is less and less due to immunizations. I suppose if you live in an area where vaccination is the devil, you may find more of this organism.
Potential Antibiotic Regimens
Age Regimen
0–1 month Ampicillin + gentamicin OR ampicillin + cefotaxime
1–3 months Ampicillin + cefotaxime/ceftriaxone
3 months–12 years Ceftriaxone ± vancomycina
> 12 years Ceftriaxone ± vancomycina
**Addition of vancomycin should be based on the regional incidence of resistant S. pneumoniae.
Regimens for Chemoprophylaxis (I will have to reformat this later)
Drug Neisseria meningitidis Haemophilus influenzae
Rifampin < 1 month old: 5 mg/kg/dose PO every 12 hours × 2 days 20 mg/kg/dose (maximum 600 mg)
> 1 month old: 10 mg/kg/dose PO every 12 hours × 2 days daily x 4 days
Adults: 600 mg PO every 12 hours × 2 days
Ceftriaxone < 15 years old: 125 mg IM × 1 dose Not indicated
> 15 years old: 250 mg IM × 1 dose
**Ciprofloxacin and azithromycin are possible alternatives although not routinely recommended.
RSV - Identify the drugs available for preventing and treating respiratory syncytial virus.
Prophylaxis
- Nonpharmacologic: Avoid crowds during RSV season and conscientiously use good hand-washing practice.
- RSV IVIG (RespiGam): No longer marketed in the United States (didn't see on the test ;))
- Palivizumab (Synagis)
- a. Dosing: 15 mg/kg/dose intramuscularly; given monthly during RSV season
- b. Effects on outcomes
i. A 55% reduction in hospitalizations for RSV
ii. Safe in patients with cyanotic congenital heart disease
iii. No reduction in overall mortality
iv. Does not interfere with the response to vaccines
v. Not recommended for the prevention of nosocomial transmission of RSV
Know this: Supportive care. Treatment is supportive care only.
American Academy of Pediatrics Palivizumab approval: (you WILL see this)
i. Premature infants born before 32 weeks’ gestation (i.e., 31 weeks, 6 days or earlier) who are 6 months old or younger at the beginning of RSV season
(a) Infants born at less than 28 weeks’ gestation may benefit up to 12 months of age.
(b) Eligible for a maximum of five doses of palivizumab during RSV season
ii. Infants with chronic lung disease who are 2 years or younger and who required medical management of their chronic lung disease in the previous 6 months – Eligible for a maximum of five doses of palivizumab during RSV season
iii. 32 and 35 weeks’ gestation (i.e., 32 weeks, 0 days through 34 weeks, 6 days) who are 3 months or younger at the beginning of RSV season
(a) With at least one of the following risk factors may benefit: infant attends childcare or sibling younger than 5 yo in same household
(b) Eligible for a maximum of three doses of palivizumab during RSV season
iv. Infants 24 months and younger with hemodynamically significant congenital heart disease
(a) Eligible for a maximum of five doses of palivizumab during RSV season
(b) There is a 58% decrease in palivizumab serum concentration after cardiopulmonary bypass; therefore, a postoperative dose of palivizumab is recommended as soon as the patient is medically stable.
v. Infants 12 months and younger with congenital abnormalities of the airway or neuromuscular disease that compromises the handling of respiratory tract secretions – Eligible for a maximum of five doses of palivizumab during RSV
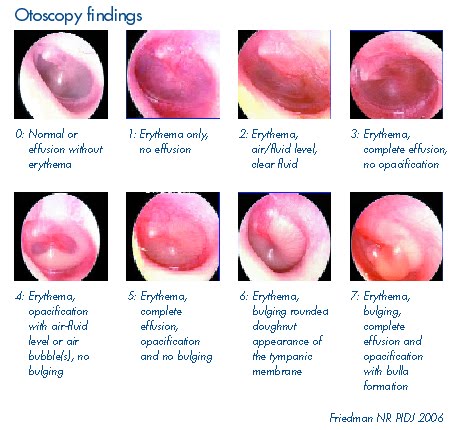
Tomorrow will continue with otitis media...



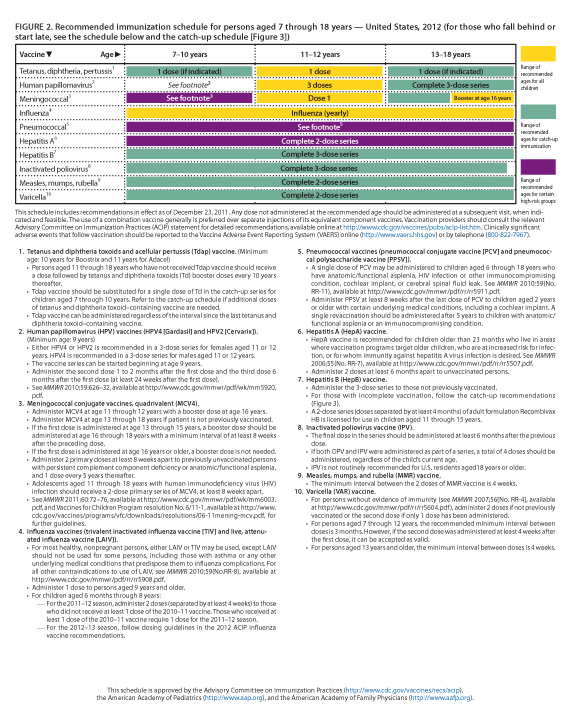
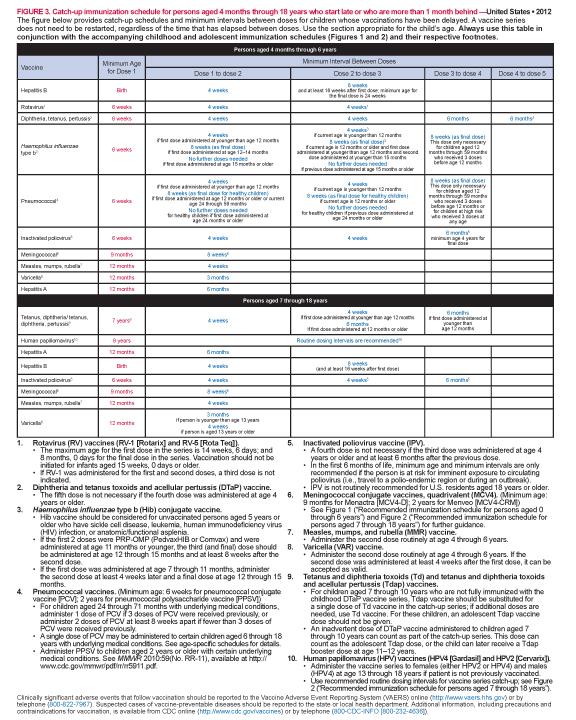
 Vaccines: the memorization of when and what and when not to if the patient has certain conditions. Imagine questions that are simple but complicated. For example, perhaps an age is given and you need to know what vaccinations were due by that age or if the child had never had vaccines what could be given as catch-up? It is really not complicated and again if you are a parent this may be an easier topic if you are of the pro-vax crowd (as I am).
Below see the schedule from the CDC that is also approved by the American Pediatric Association along with the recommended schedule for catching up on vaccines if missed.
Vaccines: the memorization of when and what and when not to if the patient has certain conditions. Imagine questions that are simple but complicated. For example, perhaps an age is given and you need to know what vaccinations were due by that age or if the child had never had vaccines what could be given as catch-up? It is really not complicated and again if you are a parent this may be an easier topic if you are of the pro-vax crowd (as I am).
Below see the schedule from the CDC that is also approved by the American Pediatric Association along with the recommended schedule for catching up on vaccines if missed.





 I am amazed daily when I am working at the hospital at the correlation between heavy weight or obesity and chronic illness. Home medication rec sheets reach pages and pages with blood pressure medications, statins for high cholesterol, diuretics, and the list goes on.
(Even sadder is the hospital cafeteria, but I have yet to dine in a hospital cafeteria and find healthy food which is odd to me)
I am amazed daily when I am working at the hospital at the correlation between heavy weight or obesity and chronic illness. Home medication rec sheets reach pages and pages with blood pressure medications, statins for high cholesterol, diuretics, and the list goes on.
(Even sadder is the hospital cafeteria, but I have yet to dine in a hospital cafeteria and find healthy food which is odd to me)